Simplified probability-theoretic evaluation of effectiveness of remote diagnostics in medicine
01/03/2019
“I saw slaves on horses. And princes walking on foot ... "No, not like that;
I saw a solar power station built under power lines.
The modern world is not a multiplication of grief because of excess of knowledge,
and raising the absurdity to even a higher power.”
.
Unknown engineer
Let us consider the death of a person, determined by the effect of marginotomy, as a timely catastrophe; and the sudden death or disability as premature. It is obvious that, using such criteria, the diagnostic value of telemedicine becomes non-zero only in case of the prevention of a premature catastrophe.
In all those cases when there is no talk of a possible catastrophe, any telemedicine immanently loses to the normal diagnostic process, which includes questioning complaints, collecting the history of the illness and life, visual examination, instrumental, biochemical, special studies. The modern clinic, against the amateur’s opinion, is a rather complicated mechanism. It is impossible to replace the standard medical routine with the transfer of pictures or video, and it is not necessary, except for some Antarctic expeditions to the pole of inaccessibility. The only real advantage of telemedicine can be considered - the gain in time necessary for making a diagnostic decision. (Perhaps, after this statement, young Internet developers and businessmen from medicine will be somewhat hurt in their best feelings, but they will somehow survive).
Let us try to formalize the statistical picture of the developing premature catastrophe. Let us consider the dependence of the probability of the survival on the time delay of the medical assistance. Naturally, we assume that this assistance can be provided only in the case of the timely solution of the diagnostic problem.
Let us synchronize the moments of the catastrophes and arrange the percentage of the survivors along the ordinate axis. On the abscissa, we will mark the delay time of the assistance. As a result, we get the desired graph of the dependence of the probability of the survival on the time, necessary for medical assistance (it would be more correct to speak of the probability density of the expectations, but this is not fundamental).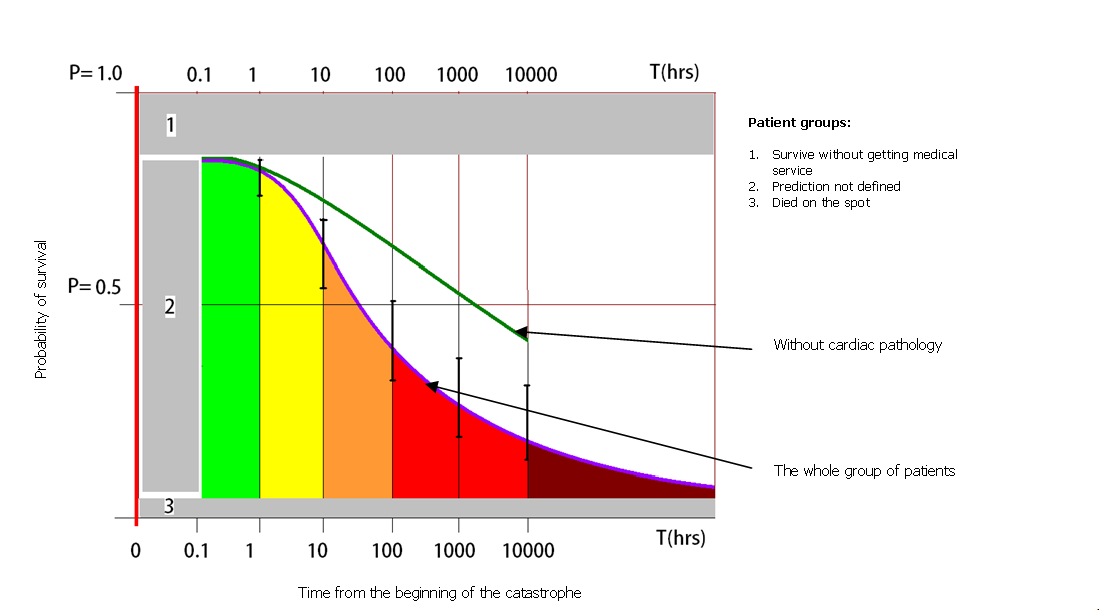
Fig.1. Dependence of the probability of the death/disability on the time of the provision of qualified assistance (explanations are in the text).
The figure shows not a graph of a function, but the simplest approximation of the statistical data (own and borrowed observations from the literature).
The area marked “3” describes the percentage of those with the immediate death (for example, accidents at speed of 200 km/h, hostilities, terrorism, etc.). The area “2” illustrates the effect of the uncertainty in the first minutes after the catastrophe (someone does the resuscitation, breaking patient’s ribs, followed by pneumothorax, many people call an ambulance, most people are at a loss, etc.). The area "1" is the percentage of the victims who will survive the catastrophe without any medical assistance.
The blue curve corresponds to the percentage of the survivors who did not receive any disability during the qualified assistance, the delay time of which is marked on the x-axis. The green curve includes statistics without cardiac pathology.
Anticipating merciless criticism, I will inform you: the author knows that the evaluation of the statistical data should be 1) unbiased, 2) reliable and 3) consistent. Of course, in this case none of these conditions is fulfilled: the graph will be completely different in the infectious focus, in the event of the outbreak of hostilities, or simply while expanding observations to other regions. But there is an undoubted advantage of such an assessment - primarily for the formation of the requirements for the technical characteristics of the telemedicine equipment.
From the graph in Fig.1. it follows that the qualified cardiologist assistance in the first hours after the catastrophe can reduce mortality/disability. This is quite expected: the empirical rule of the “golden hour” is confirmed (or rather, it confirms the correctness of our statistics). If the patient is assisted later, then its effectiveness will be significantly lower (the scale on the X axis is logarithmic, NB!).
However, it is almost impossible to deliver a cardiologist to each patient (or the patient to a cardiologist) within an hour, so the remote diagnosis in this case makes sense. For another (non-cardiologic) pathology, its effectiveness will be much lower, if any at all.
However, the remote diagnostics requires the reliable communication channel that provides guaranteed urgency, the transmission of digital quality electrocardiograms and at the same time the duplex voice contact. It is to help the consultant to get some additional information about the patient, ask the necessary questions, give advice on the ECG scanned by him, etc. Any kind of the “text communication” that has been popular among the developers lately does not replace the speech channel in any case and cannot replace it in principle. Not to mention the convenience of typing using a tablet.
Thus, a telemedicine device should be able to use all available channels: from an archaic wired telephone and analogue radio stations to modern broadband digital lines.
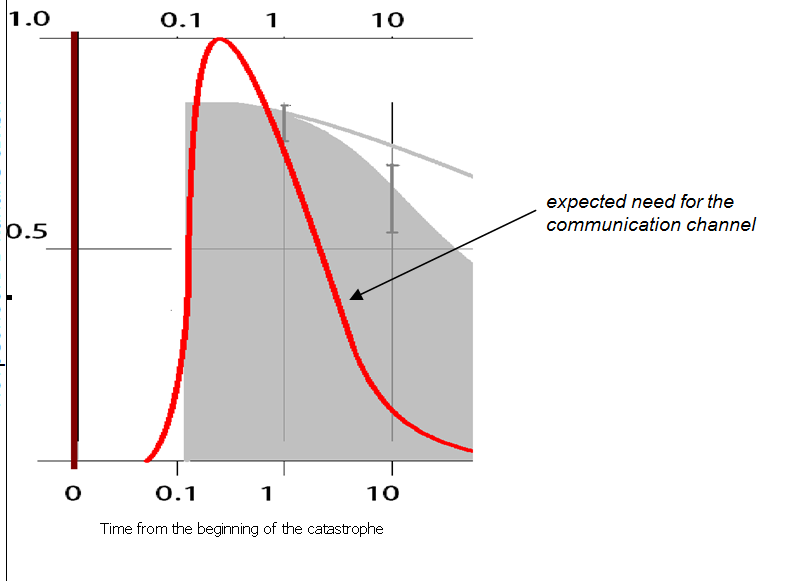
Fig. 2. The expected need for the communication channel if the teleconsultation is necessary.
The final probability of the successful teleconsultation can be described by the following formula:
Ptk - the final probability of the successful teleconsultation;
Kres - the probability of the failure-free operation of the receiving station;
Ktr - the probability of the failure-free operation of the telemedicine device;
Kline - the probability of the trouble-free communication line;
Epat - the probability of the error-free actions of the patient (his environment);
Thrs - the probability of the timely start of the qualified medical assistance;
Iadmin - the probability of the project general administration error;
n - the number of the erroneous administrative decisions.
where the “red” coefficients (the reliability of the receiver, the transmitter and the communication line), they can be improved with the help of the successful engineering solutions, and the blue “administrative” ones, which present a problem that cannot be eliminated with the help of the technical methods. Therefore, E (pat) is the percentage of the patients who visited the doctor immediately after the occurrence of, for example, the severe pressing chest pains radiating to the left arm. This percentage is small due to the existing level of the medical literacy (according to the author - no more than 25-30%), the root of which is the lack of the informational work among the population. T(hrs) is the transport delay time, which is not too large for the teleconsultation to lose its sense (i.e. in this case T(hrs) is the probability of such an event: according to different data from 0.1 to 0.25). And the coefficient I(admin) to the power n is a typical value of the contribution of the administrative error.
The resulting value of this coefficient is determined by the power n, i.e. the number of the erroneous administrative orders.
Let us explain using real examples:
1) There is no round-the-clock duty at the receiving station - coefficient 0.3, since the consultation is possible only during 8 hours out of 24 hours.
2) The ban on the transmission of the ECG, if there are no obvious and gross signs of AMI - coefficient 0.5, as, besides the fact that all painless forms will be missed, the paramedic will also minimize consultations because of understandable fears.
3) The wired telephone was disconnected for non-payment (no one from high executives even thinks about paying for traffic), the Internet is missing for the same reason, the cheap (promotional) GSM phone is no good, asking for a phone from patient’s relatives is fraught with complaint (Sic! ).
The probability that the paramedic in this situation will decide to hold a consultation is no more than 0.5.
4) It is time to do the metrology of the devices, but money for it is not budgeted. The risk of the equipment usage is passed on to users. What is the probability that they will go to the clear violation - it is unclear, but not more than 0.5?
5) The work at the central station is not paid, i.e. this is an additional burden for doctors. It is clear that they minimize the number of consultations, and nothing can be done about this. The coefficient in this case will not exceed 0.1.
6) The station was installed in the intensive care, where there is enough work even without it. Therefore, they put a nurse by the computer; she takes an ECG, prints it out and shows it to the doctor. In the event that the pathology is detected (NB!). The coefficient is difficult to be determined, because the competent nurses can be also sometimes met.
7) The most difficult case: people do not want to work for free. The administrative authorities are not going to pay. The coefficient tends to zero.
The intermediate conclusion: Any telemedicine system will have the efficiency determined by both the features of the equipment and the quality of the administration. In the ideal situation, (the administrative errors are absent), if the “golden hour rule” is implemented, the efficiency (according to our estimate) will be about 0.92 * 0.25 * 0.15 = 0.0414.
For the devices using only digital communication channels, the efficiency will be 0.0414 * 0.82 = 0.034
In the case of the non-round-the-clock operation of the receiving station, the efficiency will not exceed 0.0138.
(where, 0.92 is the probability of the correct operation of the entire ECG transmission system, including the operator errors, 0.25 is the probability that the patient and his relatives will not lose valuable time, 0.15 is the average probability that the time till the necessary operation or injection will be less than two hours, 0.82 is the coverage of the territory, providing the urgent Internet)
The obtained figures are well confirmed by the numerous medical publications: it is known that only 3% (Sic!) of the patients with acute coronary syndrome arrive to the hospital on time.
The intermediate conclusion 2: The effectiveness of the ambulance telemedicine service will always be higher than that of family doctors, dispensaries, etc. due to the lower transport delay time.
Once again, back to the formula. It is obvious that all coefficients are multipliers and, assuming their initially normal distribution, we can assume that the resulting process will be distributed lognormally.
Then, the functioning of the tree structure with the serial ECG transmission within itself will be limited to the failures, which are also distributed lognormally. It follows that the real effectiveness should be considered as the ratio of the number of the transmitted ECG for the whole period of the work to the number of the consultations required for the same period. Naturally, 4% is out of question.
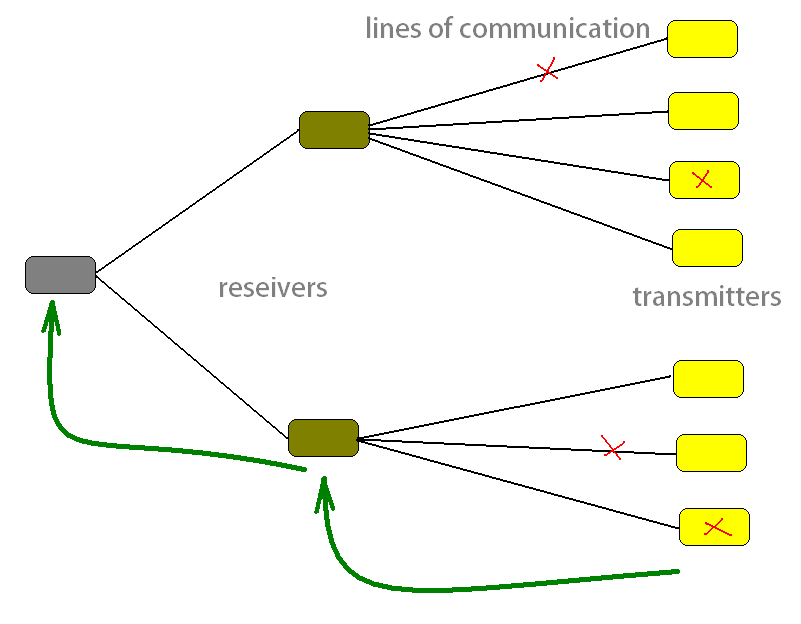
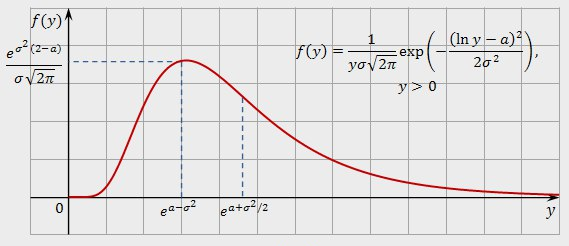
Fig.3. Typical system structure and lognormal distribution graph
Therefore, at the beginning of the work, the number of the teleconsultations will grow to its maximum, and then the degradation of the system will begin, which is described by the lognormal law. The rate of the degradation will be the higher, the more administrative errors are made, and the worse is the situation with the maintenance of the equipment. The telemedicine network left by “itself” will fail during the time approximately four times longer than the adaptation time (i.e. the maximum number of the consultation is achieved). You can stop this process only by investing additional forces and means and optimizing administrative decisions. The work of those people who, at the expense of their strength, energy and enthusiasm, support the telemedicine performance, wins admiration (we traditionally do everything not due to the thoughtful decisions of the top management, but thanks to the shoulders of the people who put their hearts into their work).
The intermediate conclusion 3: We should not expect a significant reduction in mortality and disability as the result of the implemented telemedicine system, because its effectiveness is higher the more perfect the health care system is. That is, the higher the health literacy of the population, the wider is the network of outpatient clinics, the better ambulance is provided and prepared, and the fewer amateurs are in the senior positions, the more efficient the telemedicine will be.
The final considerations will be as follows:
- Telemedicine makes sense only in cardiology, and in this respect, the Soviet developers were absolutely right. In other areas, knowingly low efficiency of the remote diagnostics is higher the sooner the results of the examination are needed.
- All types of the telemedicine kits such as “the suitcases that have everything in the world” are the waste of manpower and resources: they will only work in the field of cardiology, if they have any meaningful potential at all.
- The attempt to replace the normal medicine (which is focused on the prevention, screening examinations and the multi-level diagnostic and treatment work) with a pitiful freak with “cloud technologies” is doomed to the failure (which remains incomprehensible to the population, and even to many doctors).
The place of telemedicine is on the "ambulance’, at the link like rural ambulance stations, and in those cases when it is convenient to use it for mass preventive examinations.
Category:
- Log in to post comments
|
|
|